

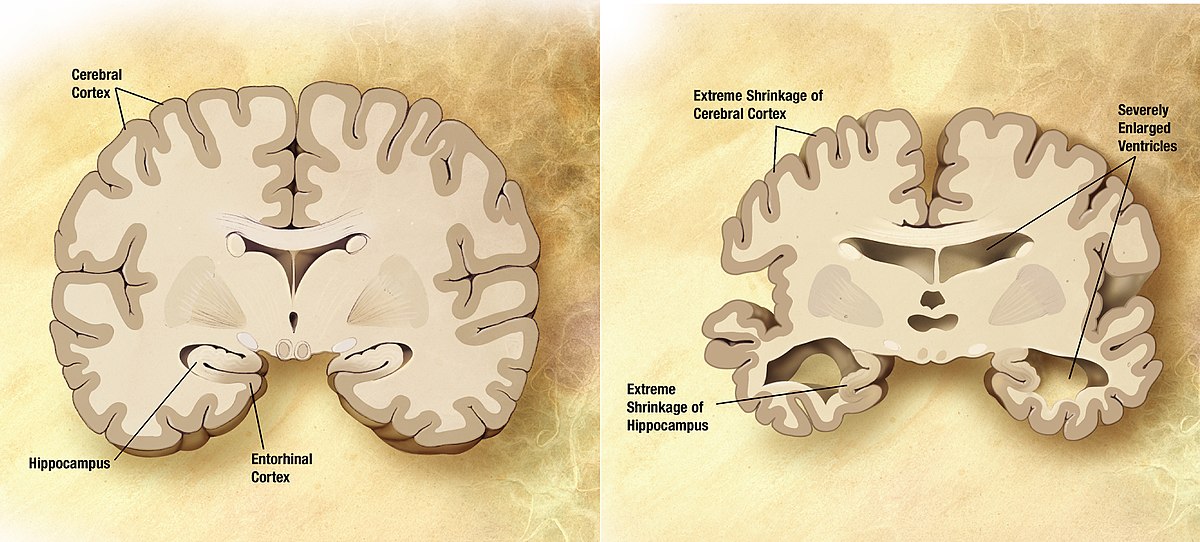
Alzheimer’s disease (AD) is the sixth-leading cause of death among adults in the US. Its progression is devastating: the brain slowly deteriorates, cognitive ability degrades, and bodily functions gradually shut down. Given our aging population and the huge financial burden of care, the National Institutes of Health is expected to contribute almost $3 billion to AD research in the year 2020 alone. Researchers worldwide have been working for decades to find a treatment. Despite their best efforts, treatments have proven mostly ineffective in clinical trials.
Some scientists now argue that the very foundation of AD research may be outdated. There is surprising evidence that AD could be triggered by an infection, rather than some intrinsic property of the brain. If true, that means decades worth of research and development may be aimed at the wrong molecular targets. Understandably, skepticism abounds among the research community. What happens when dissenting new evidence butts up against established medical paradigms?
What We Think We Know
Our current AD paradigm is based on late-1980s observations that advanced AD patients accrue massive amounts of misfolded beta amyloid (Aβ) protein peptides in their brains. Known as plaques, these protein bodies are believed to trigger further neurodegenerative processes. The amyloid hypothesis is supported by genetic evidence, as the most significant marker for predicting future AD is the APOE4 mutation. ApoE is an enzyme which helps to clear Aβ peptides from the brain, but the APOE4 variant is impaired in this activity. However, treatments designed to target Aβ peptides have never been successful.
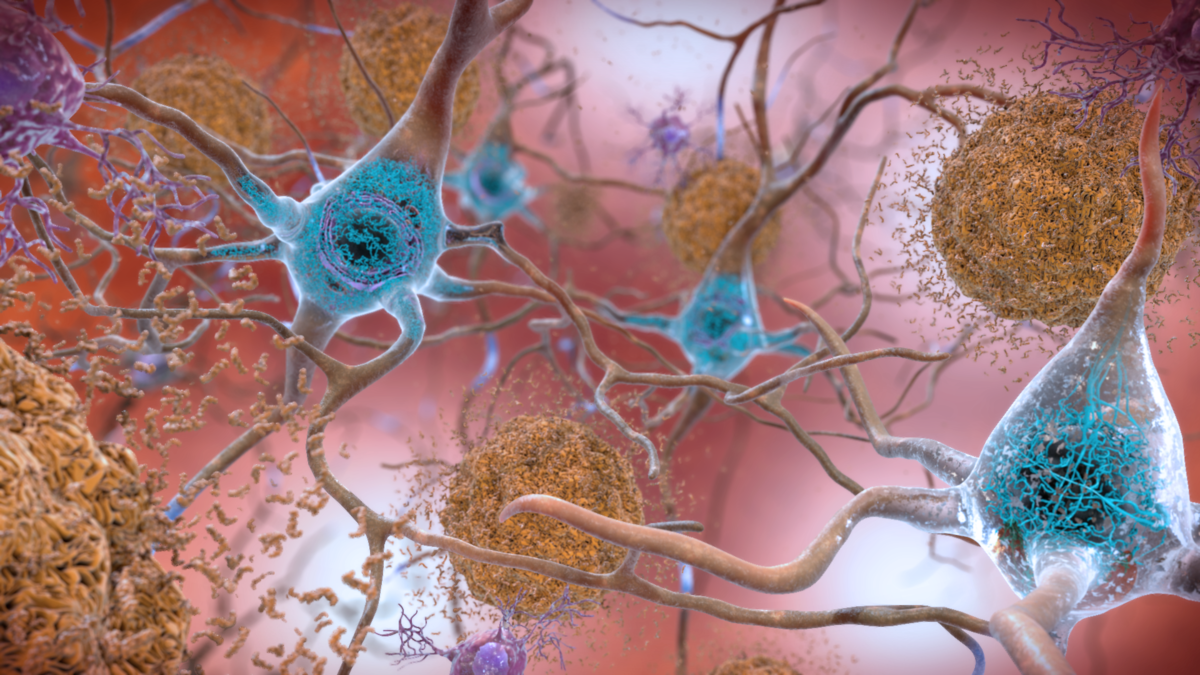
An alternative theory, the tau hypothesis, focuses on tau protein fragments that form aggregates called neurofibrillary tangles inside of nerve cells. Proponents believe that this is the biochemical cause of AD pathology. Like plaques, tau tangles accumulate in the brains of AD patients. Tau is increasingly becoming a target of new drug development, but again, clinical trials have been mostly negative.
There is little doubt at this point that Aβ and tau play important roles in AD; their near-universal prevalence in AD patients cannot be ignored. But why is it, then, that anti-Aβ and anti-tau drugs have so far proven ineffective?
A New Context for Old Discoveries
New research is providing intriguing possibilities to answer this question. Given current trends in microbiology, perhaps it is not surprising that numerous links have been proposed between AD and the microbiome. Several independent labs now believe they have identified a specific culprit: Porphyromonas gingivalis. P. gingivalis is the main bacterium involved in gum disease. What’s staggering is that this bug is able to invade the brains of ApoE-deficient mice, cause inflammation in the same brain regions that are affected by AD, and even induce production of Aêžµ plaques in the brains of previously healthy mice.
Recently, researchers found evidence of two P. gingivalis toxins in the hippocampus — the brain’s memory processing center — in 91-96% of the 54 human AD brain samples that they tested. These toxins, known as gingipains, give bacteria the ability to invade and feed on human tissues. Higher gingipain levels directly correlated with higher levels of tau neurofibrillary tangles in the human samples, demonstrating increased cognitive impairment. In a mouse model, treatment with gingipain inhibitors reduced inflammation in the brain, blocked formation of Aβ plaque components, and even rescued damaged neurons in the hippocampus. Although initial sample sizes are small, there is compelling evidence that infection may play a role in the onset or exacerbation of AD.
Changing the Paradigm?
Proposing that AD is an infectious disease seems counter to everything we’ve ever known about this illness. Assuming for a moment that this hypothesis is true, what does that mean for traditional AD research? Maybe Aβ plaques and tau bodies are not the direct causes of AD, but rather the symptoms of infection. Maybe this is why targeting these proteins has proven so ineffective. Maybe this is why there have been no significant breakthroughs in AD treatment in 40 years.
Despite the saying, science is not a perfect science. We are always bound by the limits of the information available to us at the time. What these novel studies demonstrate is that we don’t have all the information yet regarding AD. We should be willing to entertain radical new ideas that are supported by evidence, rather than hold tight to established yet fruitless paradigms. Now is a time when we can choose to be open to new ideas, or we can continue to delay life-saving advances while again confirming what doesn’t work.

About the Author

Jennifer Kurasz is a graduate student in the Department of Microbiology at UGA, where she studies the regulation of RNA repair mechanisms in Salmonella. When not in the lab, she prefers to be mediocre at many hobbies rather than settle on one. She greatly enjoys her women's weightlifting group, cooking, painting, meditation, craft beer, and any activity that gets her outdoors. She can be contacted at jennifer.kurasz25@uga.edu. More from Jennifer Kurasz.




{kind=link}